Ask Your Doctor if Capitalism is Right For You

You’re watching a football game.
It cuts to commercial: a beautiful woman twirls in a sunlit meadow. Her golden retriever runs through the grass around her. A soothing voiceover begins:
“Do you struggle with fatigue after a long day? You may be suffering from Moderate Daytime Tiredness Syndrome. Ask your doctor about Tyrexia…”
The ad goes on. And on and on and on. Somewhere around the 30-second mark, it casually mentions that Tyrexia may cause suicidal thoughts, internal bleeding, or even death.
But that part goes in one ear and out the other. The woman looks so happy. And her dog? Such a good boy!
You think to yourself, “wait a second? I do get tired at the end of the day! Maybe I should ask my doctor about this…”
This is the uniquely American ritual of prescription drug advertising - a surreal hybrid of marketing, medicine, and manipulation. It’s something most of us have grown up with. But have you ever wondered why?
The United States is one of only two countries on Earth that allow this. And if you’ve been reading Drugstore Cowboy, that should not surprise you.
Let’s take another look inside the business of American healthcare…

How Did We End Up Here?
Until the late 20th century, drugmakers focused their marketing efforts on prescribers. This was smart. Doctors controlled what medications were prescribed, and that meant sales were completely in their hands. Instead of spending on commercials, drug companies would send sales reps to prescriber offices offering samples, merchandise, expensive dinners, vacations… and likely a couple of backdoor payments. But ultimately, the only power they had to increase sales was to influence the prescribers. If you needed medication before the late nineties, you got it based on your prescriber’s clinical judgment - not because you saw a TV spot during a Friends rerun.

This is a real shirt given to doctors in the nineties to promote Xanax prescribing.

This Zoloft pen would probably sell for $150 on eBay today but doctors used to get boxes of them for free
In 1997, the FDA issued a “clarification” to its advertising rules: drug companies no longer had to include every side effect in broadcast ads. They could now list only the most significant risks - so long as they directed viewers to a phone number, website, or print ad with full details.
I call that moment the “Big Bang of Big Pharma Advertising.”
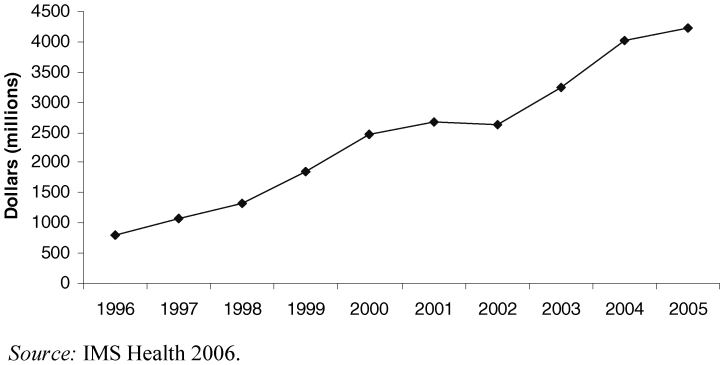
Total U.S. Pharmaceutical Industry Spending on DTCA 1996–2005
It opened the door to modern DTC (direct-to-consumer) pharmaceutical advertising, shifting the focus of marketing from prescribers to consumers. This is what finally allowed marketers to sell prescription drugs like consumer goods… as long as there was just enough fine print to keep regulators at bay.
By the early 2000s, we had entered a new era: the blockbuster ad-driven drug. Many of you are old enough to remember commercials for these “miracle drugs”:
Celebrex. Lunesta. Abilify. Nexium. Viagra. Just to name a few…
All household names - not because of their clinical data, but because they were advertised on prime-time television with carefully crafted emotional appeal that led to sales never seen before in the pharmaceutical industry.
We are the only developed country that thinks it’s appropriate to advertise prescription drugs on television. The primary result is increased demand for expensive brand-name drugs that may not be appropriate or necessary.

Khloe Kardashian promoting Nurtec. One of many, many celebrity pharma spokespeople.
The Fair Balance Farce
The FDA does require “fair balance” in prescription drug ads - meaning companies must present risks and benefits in equal measure. But in practice, this has become a joke.
The trick is simple: Show beautiful people. Speak softly. List the dangers in a gentle monotone while images of smiling couples, family reunions, or happy dogs play in slow motion. Finish with the most serious risks being read by an auctioneer.
I don’t even have to show examples. Every one of you reading this knows exactly what I’m talking about.
Oh - and don’t forget about the music! My personal favorite: “Oh-oh-oh-OZEMPIC!”
The message isn’t “this drug might cause internal bleeding.” The message is “you’ll finally be happy again!”
And, of course, it works. A 2018 study found that patients exposed to DTC drug ads were more likely to request a specific brand by name regardless of whether it was clinically indicated.
Even doctors are influenced. When patients come in asking for “that drug from TV,” the path of least resistance is often to prescribe it - especially in a rushed clinical setting. With doctors feeling more overwhelmed and overloaded with patients than ever before, you can’t blame them for just giving a patient what they ask for if it keeps them placated and coming back for another visit.
And in the ever expanding world of concierge medicine - where patients can pay tens of thousands of dollars a year for access to a specific doctor - the line between patient and customer can be damn near indistinguishable. Those prescribers have no choice but to give their patients what they want… or risk losing their business.
Where the Money Goes
If you’re wondering how much drug companies spend to maintain this illusion, the answer is… a lot.
In 2023, the pharmaceutical industry spent nearly $14 billion on DTC ads in the US.
Here are a few examples:
AbbVie spent $580 million on Skyrizi alone (one drug!) They spent an additional $495mm+ on Rinvoq, and $162mm+ on Vraylar.
Sanofi spent $502 million just on ads for Dupixent
Takeda spent over $226 million promoting Entyvio
To put that in perspective:
Nike spent roughly $3.9 billion globally on all marketing in 2023
Coca-Cola spent $4.4 billion
Apple spent about $3.1 billion
But those are global totals (taken from their 2023 10-K filings). The drug companies above spent their billions in the US only - and just on consumer-facing prescription ads. These are astronomical numbers.

Big Pharma is just a different animal.
And while Big Pharma claims to invest heavily in R&D, watchdogs like Public Citizen have pointed out that some companies spend more on sales and marketing than they do on actual drug development.
Cue my weekly line: “Healthcare is a business”
When the Rules Don’t Apply: Telehealth and the Loophole Economy
If all this sounds crazy enough, consider this: these rules only apply if you’re advertising an FDA-approved drug.
The moment you step into the world of compounded medications or telehealth startups, everything changes.
Compounded drugs are not FDA-approved. That means they haven’t been reviewed for safety, effectiveness, or quality. And as a result, they’re not subject to the same promotional restrictions as branded pharmaceuticals.
“Because compounded drugs are not FDA-approved, they have not been reviewed by the agency for safety, effectiveness, or quality. Advertising of compounded drugs may be false or misleading if it implies FDA approval or omits material information about risks.”
In practice, this means compounders can:
Skip the long disclaimers and “fair balance” rules
Market their products as “custom formulas” or “personalized treatments”
Use lifestyle or wellness language to sidestep risk-heavy terminology
The same goes for telehealth platforms. Companies like Hims, Ro, and Eden position themselves as digital health services - not drug manufacturers. This allows them to:
Avoid preclearance from the FDA’s Office of Prescription Drug Promotion
Frame prescription access as part of a broader lifestyle offer
Use glossy Instagram-style campaigns that feel more like fashion ads than medical guidance
There’s a loophole here and they know it.
When Eli Lilly runs a TV commercial for semaglutide, they’re required to spell out the black box warnings. But if a compounder markets a compounded GLP-1 through a telehealth platform, they can call it “a customized weight loss solution” and link to a checkout page. No warning letters. No fine print. No fair balance.
“Compounded drugs are not subject to premarket review or approval by FDA, and therefore are not subject to the same labeling requirements as FDA-approved drugs,” the agency states.
It raises a deeper question:
Are we regulating the message? Or just the messenger?

Should We Ban It?
I’ll be fair today. There are arguments on both sides of this.
Critics say DTC ads:
Encourage overprescribing and overtreatment
Medicalize ordinary life (e.g., “social anxiety disorder” or “low T”)
Raise drug prices (not just for consumers, but for the government’s bill as well) by promoting expensive brands over generics
Undermine the doctor-patient relationship
Defenders say:
Ads raise awareness of underdiagnosed or stigmatized conditions
They empower patients to initiate important conversations
They normalize treatment for real issues like depression, HIV, and erectile dysfunction
Both sides are partially right. But here’s what’s undeniable:
We’ve normalized something the rest of the world rejects.
Only one other country - New Zealand - allows it. And they’ve nearly banned it multiple times. In 2006, a government review found that DTC advertising led to higher costs and overuse of certain drugs. In 2011, their health minister called it “an experiment that failed.”
In the US, RFK Jr. has recently suggested banning DTC pharmaceutical ads altogether. It’s unlikely to gain traction this election cycle - but the fact that it’s even being discussed shows growing skepticism about the practice.
After all, we’ve banned cigarette ads. But Big Pharma can advertise an injectable immunosuppressant with a black box warning as long as there’s a puppy in the background and a piano score.

A Final Dose of Clarity
To be honest, I still don’t know exactly where I stand on this issue. What I do know is that pharma advertising is the strongest representation of how the healthcare system in America intersects with capitalism. My goal today - and always - is just to get you thinking about something you haven’t thought about before. Whatever your view, it’s worth asking why every other developed country has drawn the line - and why we haven’t.
So, here’s my challenge for all of you. The next time you hear those familiar words…
“Ask your doctor if [X] is right for you…”
try asking a different question:
“Why am I being sold a prescription in the first place?”
Saddle up.

Alec Wade Ginsberg, PharmD, RPh
4th-Gen Pharmacist | Owner & COO, C.O. Bigelow
Founder, Drugstore Cowboy